FACT OR FICTION?

May 2001
Written By
W. Azul La Luz
Sociology Department
Ph.D. Student
University of New Mexico
Albuquerque, NM
TABLE OF CONTENT
Written By
W. Azul La Luz
Sociology Department
Ph.D. Student
University of New Mexico
Albuquerque, NM
INTRODUCTION
Why Study Latinas?
Paucity Of Research
How the Paper is Organized
THEORETICAL PERSPECTIVE
Historical Perspective
Medicine In Latin America
Theoretical Grounding
Epidemiology
and Social Epidemiology In the United States
Epidemiological Paradox
Bringing It Home To the
United States
The Heart of the Matter To
Summarize
IDENTIFYING THE TARGET
GROUP
Who Are These Latinas and Latinos?
Table One:
Latina and Latino population in the USA, 2000
Table Two:
National Distribution of Latinas and Latinos, 1999
Table Three:
States with the Highest Concentrations of Latinas and Latinas, 1999
Latinas
Table Four:
Latinas In the United States, 1995 TO 2000
Disaggregation
Whetting the Senses:
Latinas in Prison
LATINAS'
EPIDEMIOLOGICAL PARADOX
All Against Speak
Now
In Opposition: Stroke
In Opposition: Diabetes
In Opposition: Cancer
In Opposition: Physical Disability
In Opposition: Health Insurance
and Access
All in Favor Speak Now
In Favor: Heart Disease
In Favor: Mother and Child Outcomes
In Favor: Mental Health
In Favor: Cancer
In Favor: Culture Confianza
A Qualitative Example
In Summary
TOWARDS A METHODOLOGY
Future Direction
Why
Study Latinas?
Latinas in the United States
are a large and unique ethnic group (1)
that bear critical research. Why should research about Latinas be done?
I submit that there are, at very least, four important reasons.
Paucity
Of Research
Despite the population size
of Latinas in the United States, their relatively large numbers have not
engender adequate academic curiosity leading to substantial scholarly research.
Research into Latina issues is a relatively new phenomenon in the United
States. Serious and rigorous research on Latinas as a distinct sociological
group, appears to have begun in the early 1980's (Sorensen and Siegle,
1992). Latinas have been virtually non-existent historically in the health
literature in the United States before then.
The paucity of rigorous
(or even soft) research in all the social sciences with regards to all
aspect of Latinas' lives is appalling. What small amount there is mostly
surrounds birthing, and much of the research is contradictory (Cofer, 2000;
Hogue, et al, 2000; Lambety and Coll, 1994). It is as if Latinas were only
a human reproductive system.
Them Latinas' situation
in the United Sates cries out for new and varied research, particularly
epidemiological research from a social medical perspective. This paper
is an attempt to begin a narrative in that direction.
How
the Paper is Organized
In the next section, Theoretical
Perspective, presents a theoretical framework grounded in social medicine.
It includes a strictly abbreviated and interpretive, outline of the modern
history of medicine in the United States and Latin America. It also includes
a dialogue on epidemiology generally, and specifically relative to social
medicine and Latinas.
Some characteristics of
Latinas are laid-out in the third section, Identifying the Target Group.
There is no attempt to flesh-out who the Latinas are in the United States,
their place of origins, or variations in culture. Nor is there any qualitative
or quantitative accounting of risk factors. These are accepted as given
for all the studies. The analyses of both these topics will be necessary
in a more exhaustive treatment of the Latina issues, such as my dissertation.
The fourth section, Latinas'
EP, is divided into two subsections. The first subsection examines some
postulated theories and research that has either attempted to disprove
or prove that an EP exist with regards to Latinas. This section is not
meant to be definitive. The section merely attempts to demonstrate
some of the confusion and controversy surrounding the issue. The second
subsection gives a qualitative example of one Latina's life which I believe
epitomizes the Latinas EP in the United States.
The last section discusses
and concludes the paper with an eye towards a methodology that may be used
to test the hypothesis presented: the EP is an irrelevant misinterpretation
of political, social, and class factors.
Historical
Perspective
The illness sciences in
the United States have followed, with minor deviations, the same linear
capitalistic movement as the rest of the "manifest" market expansion through
ideological legitimation. In the early to mid nineteenth century social
medicine, chiropractic, and homeopathy, were all part of the nascent medical
fabric in the United States. However, all these gave way to the capitalistic
pressures of the market place and the ruling medical colleges, namely John
Hopkins.
As a direct consequence
of the Flexner Report (1907) (which posited unproven universities) John
Hopkins University, under the auspices and encouragement of the Rockerfella
Foundation, consolidated the power of the unifactorial, disease model (Waitzkin,
2000).
The American Medical Association
(AMA) consolidated its powers with the help of the elite coming from Harvard
and John Hopkins universities and established its hegemonic roll by the
early 1900's. By 1920, the AMA had established national codification of
board certification and state licensing through its state elite-dominated
branches. Concurrently, market expansion encouraged exclusivity and congregating
medical practices into large growing urban areas. Further, as a direct
consequence of the facility afforded by cars and telephones, a"sovereign
professional" class was created and firmly entrenched by the middle of
the twentieth century (Starr, 1949).
The medical establishment's
entrenchment has dominated until today with medicalization of virtually
every aspect of life. An excellent example of medicalization is human reproduction.
Before medicalization of the birthing process, there was prestige for midwives,
and curanderas who were almost entirely women - I helped my mother deliver
several babies with very little or no problems. After medicalization, the
entire reproduction process became the total domain of mostly male doctors.
Every aspect of human reproduction has been medicalized from fertilization
to feeding the new born (Freund and McGuire, 1999). Every aspect of a women's
reproductive cycle, from menstruation to menopause have become the province
of mostly male doctors. As a consequence, female processes are described
in terms of illness while men's are described in terms of virility and
robustness (Reagan and Willis, 2000).
With the advent of the human
"rights" movements of the 1950's an1960's - civil, prisoners's, sexual,
women's, - there has been some concession to social factors, such as race
and ethnicity (Fanion, 1963) and work stress and status (Jackal, 1977;
Karasek and Theorell; Freund, 1982, 1990, 1998). However, the "medical
industrial complex" still dominates. This is evident in the proliferation
and exportation of health management organizations (Relman, 1980; Iriart,
Merhy, Waitzkin, 2001).
There is currently even
a conservative movement to eliminate the little progress that has been
made in the area of social determinates, civil and other rights: gains
in human rights are viewed as invasion of the medical kingdom by the serfs
(Satel, 2000).
Medicine
In Latin America
In Latin America the medical
story developed much differently than in the United States. The mid Nineteenth
Century to the early Twentieth Century saw the inception of hegemonic medicine
in the United States, with a concomitant suppression of all other forms
of medical thought. At the same time, in Latin America social medicine
saw its inception and nourishment.
The foundations of social
medicine in Latin America came directly from pathologist such as Max Westenhofer
who studied in Germany primarily under Rudolph Virchow. Some credit is
also given also to Eugenio Espejo, a Spain Physician, who independently
came with similar conclusion as Virchow. Nonetheless,Virchow, a Germany
pathologist, whose multifactorial analysis of health and disease concatenating
poverty and communicable diseases, such as typhus, is given much of the
credit for being the father of social medicine in Latina America (Waitzkin,
2000).
Virchow was intimately familiar
with the pioneering work of Fredick Engels with regard to Engels' investigation
of living quarter conditions and factory related disease causation, such
as the relationship between tuberculosis and typhus and socioeconomic and
environmental factors. Building on Engels' work, Virchow engendered the
notion that pathology responds to constitutive change in society and thus,
he birthed social medicine (Waitzkin, et al, 2001; Waitzkin, 2000).
Virchow defined the new
field as "social science," a term still used today in Latin America. He
presented compelling statistical data and observation on pathology to buttress
his arguments. These observations and significant investigations were extremely
influential, to the point that his work, along with his political activism,
were instrumental in the Germany reform movements that in 1848 brought
about a revolution (Waitzkin, et al, 2001; Waitzkin, 2000).
In Latin America, directly
influenced by Virchow's, and later by Liberation Theology, Empowerment
Education, and a number of other educational and grass roots initiatives,
social medicine blossomed from the late Nineteenth Century to the present
day. Admittedly there have been periods of intermittent repression by the
state, particularly in the 1960's and 1970's, in many countries including
Argentina, Brazil, and Chile. Despite these periodic setbacks, there have
been many influential figures that have contributed to social medicine
in Latin America. Such people as Luis Emillio Recabarren, Salvador Allende,
Juan César Garcia, María Isabel Rodriguez in Chile; Juan
B. Justo, in Argentina; Ernesto "Che" Guevara, in Cuba and elsewhere in
Latin America; Pablo Arturo Suárez, and Ricardo Paredes in Ecuador;
Camilo Torres in Colombia; and Frei Betto in Brazil.
Currently, there are a number
of progressive groups in Latin America based in Argentina, Brazil, Chile,
Ecuador, and Mexico who continue to propagate and fight using social medicine
as a tool for the progress of the labor class (Waitzkin, et al, 200).
Theoretical
Grounding
Unlike Unitedstatian medicine,
a particular aspect of social medicine is its grounding in theory. Its
research and methodologies are a direct result of its theoretical perspective,
and in turn hone its theory by continuously reevaluating in light of application
outcomes (Waitzkin, Iriart, Estrada, and Lamadrid, 2001; Waitzkin, 2000,
Breilh, 1995; Laurell 1989).
In the United States the
dominant singular view is that germs and other pathogens cause disease,
and as such disease is an individualistic causation and cure model. This
view prevails even when dealing with the effect of epidemics on myriad
individuals. This unifactorial view is in direct contrast to social medicine.
Social medicine espouses the theoretical view that one of the most important
cause of illness and health are the "material conditions of people's everyday
lives... [and] ... an effective health-care system cannot limit itself
to treating the pathophysiologic disturbances of individual patients."
Effective development of health-care systems must encompass basal changes
in economic, political, and social conditions (Waitzkin, 2000, 38).
Also in sharp contrast to
social medicine is the Unitedstatian (4)
market driven, individualistic technocratic, therapies and the antithetical
epidemiological approach, whether clinical or social. In contrast, social
medicine epidemiology embraces a methodology that is life encompassing
and historical (Breilh, 1995; Laurell, 1989). This is explained in more
detail in the section to follow.
Epidemiology
and Social Epidemiology In the United States
In the United States, epidemiology
is the art of projecting incidence and prevalence of illness events over
a given period of time and for a specific population of individuals. Social
epidemiology is the particular ideologies that form the Unitedstatian health
sciences' underpinnings of human illness (Lupton, 2000; Armstrong, 2000),
and which are used as one of the primary control methods of dominant medical
thought (Breilh, 1977; Laurell, 1989). The sociological dimension of health
and illness interact with United States hegemonic medicine, or circumvent
it altogether, depending on one's theoretical outlook. Various elements
become important in the dominant epidemiological discourse, such as aging
(Estes and Linkins, 2000), culture (Trotter, 2000), gender (Lane and Cibula,
2000), geographic landscape (Catalano and Pickett, 2000), and socioeconomic
status (Robert and House, 2000), but in all cases, it is an individualized
perspective.
That is, Unitedstatian social
epidemiology attempts to explain health and illness trends in groups and/or
populations from the dominant social context regardless of the group it
is researching. Further, it treats social factors as superficial at best,
or takes then for granted as common sense (Laurell, 1989). An excellent
description of this may be found in research on hypertension by Schnall
and Kern (1986) in which they explain the failure of hegemonic medicine
to provide adequate genesis for hypertension, and they provide an excellent
historical analysis relating it to the stress of modern society.
As such, from the prevailing
and currently dominant medical framework in the United States, epidemiology
is an indispensable tool of Public Health because it allows public health
providers to intervene in individualistic illness progression or in designing
prevention programs and interventions from a medical and social perspective
(Lupton, 2000; Armstrong, 2000; Fairbanks and Wiese, 1998). For example,
childhood inoculations, needle exchange programs for IV drug users, anti-drinking
and driving campaigns, or prostitution licencing to prevent spread of STD
through illegal prostitution. Epidemiology also helps public health providers
to propagate good health habits: well baby clinics, nutrition fairs, breast
cancer screening, hand washing campaigns generally, and particularly in
handling food, etc. In truth, much that passes for medical improvement
outcomes, turns out to be historical antecedents to the improvement: tuberculosis
decline with societal improvement with little regard to medical advances
(Waitzkin, 2001).
Epidemiological
Paradox
If grounded in theory, another
avenue of discourse epidemiology provides the entire field of health and
illness is "food for thought," equivalent to the purpose philosophy discharges
relative to the "hard" sciences generally. Both Unitedstatian and in Latin
America epidemiology seem to lead the way in health science by identify
unusual phenomena. One such thought-provoking, and unusual epidemiological
phenomenon is any EP: an a priori expected health or illness outcome
that does not occur, and actually has an unexpected and/or opposite
(or lower or higher) outcome than is predictable from the observable facts
or variables.
There is an EP surrounding
health and illness, and other social elements to do with Latinas in the
United States. Latinas exhibit excellent health and illness outcomes relative
to AA women and EA women. This, despite alarming discrimination, predominate
lower class status employment, and exhibition of other high risk factors
that should lead to poor health outcomes. This has been termed the "epidemiological
contradiction" or "epidemiological paradox" (Cervantes, 1996, p3). This
EP has also been found in Latina's incarceration patterns (La Luz, 1997).
Bringing
It Home To the United States
From another perspective,
what is more important to the collective health/illness analysis is a dialectic
formed from historical materialism and social medicine. As such, the intersection
of class, culture, gender, race, and politics, overarched by the means
of production, are the epidemiological direction of social medicine. Therefore
any analysis undertaken must take into account every aspect of the entire
group being analyzed (Breilh, 1995; Laurell, 1989).
Social medicine or collective
health... postulates the necessity to analyze the health and disease phenomena
in the context of the economic, political, and ideological process of society
and not just as biological phenomena that concerns individuals..." (Laurell,
1989, 1183)
When examined through the
lenses of social medicine, there may not exist an EP in Latinas
in the United States. While the EP, as presented, is controversial and
unproven, it has come to be accepted as hegemonic medical ideology. Though,
in point of fact, it has neither been completely demonstrated as a reality,
nor completely disproved. I discuss this in more detail in the next section,
when I review of some of the literature.
However, to press on with
the theoretical, if we accept, for the sake of argument, that the EP exists,
it has been explained as a function of the Latina and Latino experience.
However, it may actually be a generalized theoretical construct caused
through a mis-interpretation of the facts from a functional medical perspective.
Other explanations of the EP using dominant ideological social epidemiological
constructs that have been offered are:
The
Heart of the Matter
It has been pre-supposed,
a priori, by the dominate epidemiology, that Latinas evidence the same
risk factors as the other females in the United States - EA and AA women.
Even more important, it has been assumed that Latinas' health outcomes
had the same relationship to these risk factors as do AA and EA. These
risk factors defined by the Unitedstatian hegemonic medical/scientific
establishment, are rendered meaningless with relationship to Latinas because
the risk factors have been studied out of there respective collective historical
dialectic: the intersection of production, reproduction, class and gender.
For example, low paying,
low status employment, is correlated with poor health outcomes in EA and
AA (and even for acculturated Latinas). Employment of this type may be
meaningless as a risk indicator of health outcomes for Latinas who are
not acculturated to the Unitedstatian life styles. Employment that in the
United States is considered low income and low status, may not be considered
either by Latinas. Such "low status" employment, under different political,
social, and class perspective may actually be prestigious and may provide
a comparatively high standard of living, or quality of life wages not perceived
as such by the dominant capitalistic culture.
United States consumer status
and reproduction mechanisms are closely tied to worker stratification and
alienation. This may not be the case for first generation Latinas and Latinas
living in enclave or colonias. In short, Latinas' health outcomes in the
United States have been measured through a faulty hegemonic medical paradigm,
instead of through their own collective self and group perception with
its interrelation to all other ramifying factor of class, gender, race,
and politics.
A complete analysis and
synthesis of these issues are far beyond the scope of this paper and will
be fully constructed within my dissertation. However, an abbreviated directional
overview of the main issues pro and con follows. This will be done with
an eye towards the development of instruments that may be used in collective
and individual interviews to gather the predictive data. Data that, I believe,
will demonstrate that an EP only exist as it relates to the majority culture,
but disappears when viewed from the Latina perspective.
I do not fail to see the
dangerousness of this argument. That is why, I hasten to add that even
if my inferences are correct, it should not be used as a method of continuing
to oppress and subjugate Latinas, particularly new arrivals to the United
States. Instead we need to look at the salubrious side of the finding for
replication and see how they eliminate social contradiction such as internalized
racism, and reproduction.
To
Summarize
In short, social medicine's
analytical tools have not been used much in the United States and are not
well know. I posit that if we use the social science epidemiological approach
to analyze the current controversy, the EP surrounding Latinas in the United
States, the outcome of such an analysis would be, I believe, a totally
new understanding of the Latinas' location in the United States stratification
structure. The risk factors will cease to be such, transformed by the Latina's
own world's view, into something far more insidious and dangerous.
Who
Are These Latinas and Latinos?
Before exploring the risk
factors and health and illness outcomes, it is necessary to write about
who Latinas are in the United States. However, it was somewhat difficult
to obtain accurate and exact numbers of Latinas as a distinct population
subgroup. It is even more difficult to obtain disaggregate numbers of the
Latina subgoups in the United States, namely, Mexican, Puerto Rican, Cuban,
Dominicans, etc. I attempt to present a picture of Latinas and Latinos
generally, then one about Latinas in particular as an extract from the
numbers given.
As may be seen in Table
One below, according to the United States Census Bureau (2000), in 1999
Latinas and Latinos in the United States (USA)accounted for about 32.7
million people or about 11.7 percent of the entire population, excluding
the United States colony of Puerto Rico. This 11.7 percent was made up
of approximately 65.2% Mexican, 14.3% Central and South American, 9.6%
Puerto Rican, 4.3% Cuban, and 6.6% other Latina and Latino peoples (US
Census Bureau, 2000).
Table
One: Latina and Latino population in the USA, 2000
| Total and Disaggregate | Total numbers | Percentages |
| All Latinas and Latinos | 35,305,818 | 11.70% |
| Mexican | 23,019,393.34 | 65.20% |
| Central and South Americans | 5,048,731.97 | 14.30% |
| Puerto Rican | 3,389,358.53 | 9.60% |
| Cuban | 1,518,150.17 | 4.30% |
| Other Latinas/Latinos Peoples | 2,330,183.99 | 6.60% |
| Total | 35,305,818.00 | 100.00% |
Table
Two: National Distribution of Latinas and Latinos, 1999
| Region of the United States | Latina and Latino Population | Percentage |
| Totals | 35,305,818 | 100.000% |
| Western States | 15,340,503 | 43.450% |
| Southern States | 11,586,696 | 32.818% |
| Northeast States | 5,254,087 | 14.882% |
| Midwestern States | 3,124,532 | 8.850% |
Table Two above shows
the distribution of Latinas and Latinos by Geographic Region in the United
States. Approximately 44% (13,983,000) of Latinas and Latinos lived in
Western States, 33% (10,391,000) in the Southern States, 16% (4,909,000)
in the Northwest States, and 8% (2,406,000)in the Midwest States.
As may be seen in Table
Three below, in 1999, which is the most recent Census Bureau offers in
this regard, New Mexico was the state that had the highest concentration
of Latinas and Latinos (where Hispanics constituted 40 percent of the total
population). Following New Mexico were California with 31 percent, Texas
with 29 percent, Arizona with 22 percent, figures that the USA Nevada with15
percent, and Colorado, Florida and New York with 14 percent (US Census
Bureau, 1999).
The majority of Latinas
and Latinos live in rural or non-metropolitan areas. Of the numbers represented
in Table One, Two and Three, some 52%, or about 16,484,000 million Latinas
and Latinos in the United States live in rural or non-inner city areas.
The other 48% (15,216,000) live in inner city areas of the USA (US Census
Bureau, 2000, 1999).
Table
Three: States with the Highest Concentrations of Latinas and Latinas, 1999
| State | Total Latina and Latino Population in State | Percent of State Population |
| Arizona | 1,056,011 | 22.10% |
| California | 10,274,988 | 31.00% |
| Colorado | 588,139 | 14.50% |
| Florida | 2,266,687 | 15.00% |
| Nevada | 287,671 | 15.90% |
| New Mexico | 701,157 | 40.30% |
| New York | 2,620,310 | 14.40% |
| Texas | 5,953,110 | 29.70% |
As Table Four below shows, there are approximately 16.3 million Latinas in the United States. They are, as a population, relatively younger than EA women, and bear considerably morechildren within their fertility window (LatinMed.com, 2001). They are also a minority twice over: in the United States is here are less Latinas (16.3 million females) than there are Latinos (16.4 million males). All other peoples in the United States have more females than males. There has been no definitive answer for this fact. It is possible that this demographic fact is due to more Latinos than Latinas immigrating to the United States (La Luz, 1997), but that has not been definitively explained in any research.
Table
Four: Latinas In the United States, 1995 TO 2000
| HISPANIC ORIGIN (of any race) | 2000 | 1999 | 1998 | 1997 | 1996 | 1995 |
| Population | 32,734 | 31,337 | 30,252 | 29,182 | 28,099 | 27,107 |
| (Percent of total) | 11.90% | 11.50% | 11.20% | 10.90% | 10.60% | 10.30% |
| Male population | 16,442 | 15,761 | 15,233 | 14,716 | 14,193 | 13,713 |
| Female population | 16,293 | 15,576 | 15,018 | 14,466 | 13,906 | 13,328 |
| Female % of all Hispanics | 49.774% | 49.705% | 49.643% | 49.572% | 49.489% | 49.168% |
| Female % of all Females | 11.558% | 11.172% | 10.865% | 10.559% | 10.246% | 9.909% |
| Female % of entire population | 5.907% | 5.712% | 5.557% | 5.402% | 5.243% | 5.071% |
In Opposition: Diabetes
Diabetes in Mexican-Americans is two to five times
more prevalent than among other minorities in the U.S. Of the 30 million
Latinas and Latinos in the United States in1998, some 1.2 million were
diagnosed with diabetes, and it was estimated that as many as 675,000 went
undiagnosed. Being overweight is a major risk factor for diabetes and Latinas
and Latinos are more at risk for being overweight than EA in the United
States (Flagg,1999; Hazuda, Haffner, Stem, and Eifler, 1988; Samet, Coultas,
Howard, Skipper, and Hanis, 1988).
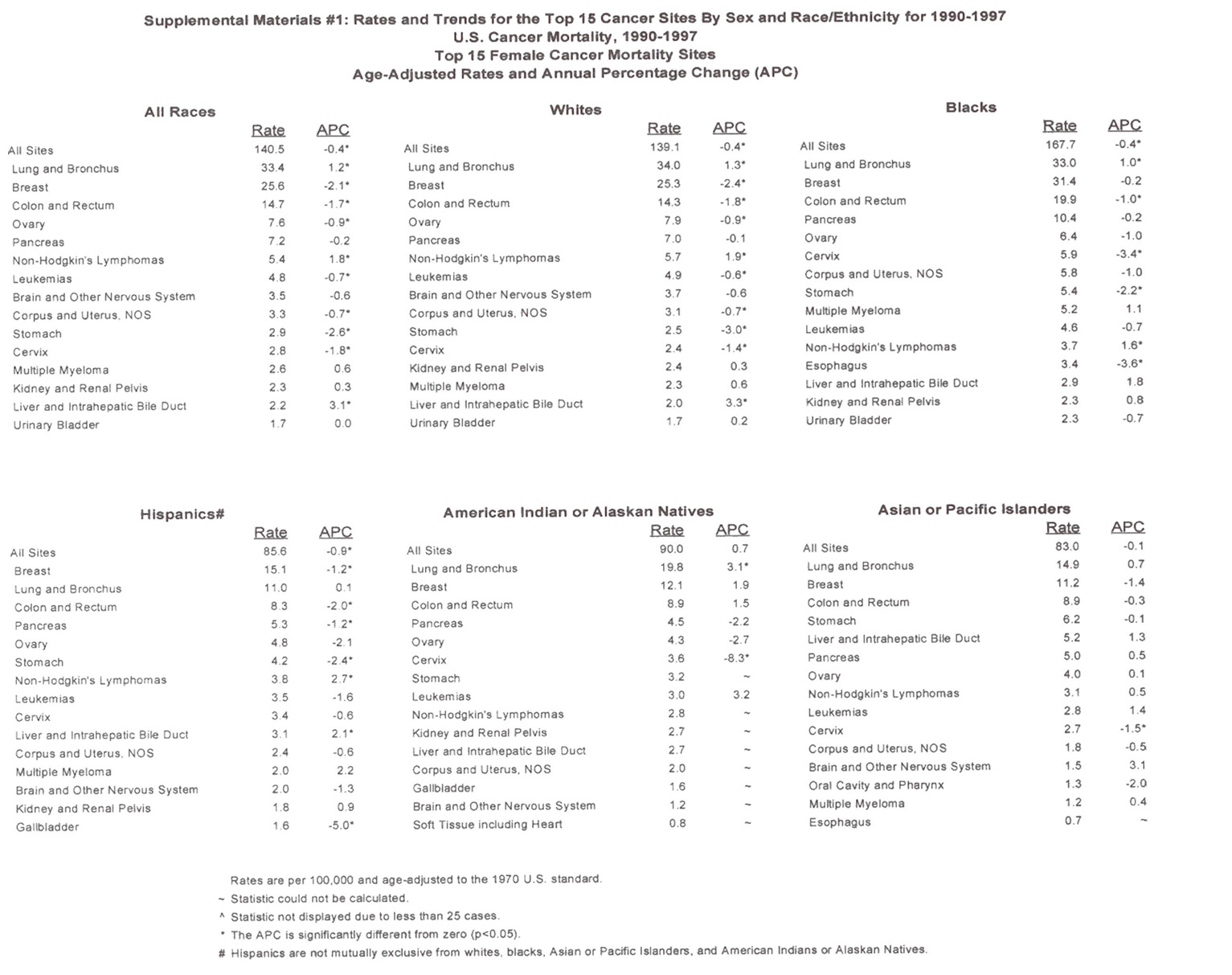
In Opposition: Cancer
Latinas' five-year breast
cancer survival rate (70%) is far worse than for EA women (84%). This is
due in part to late diagnosis. Latinas tend to not seek medical attention
until they present with severe symptoms (Flagg,1999). Additionally, comparison
of records in New York City between 1969 to 1971 and 1979 to 1981 showed
that Latinas born in the United States had higher rates of stomach and
cervical cancer than EA women (Rosenwaike and Shai, 1986).
In several other studies,
Latinas of various ethnic subgroups - Columbian, Ecuadorian, Dominican,
Mexican American, and Puerto Rican - were as likely as EA to develop breast
cancer, were more likely to die of it, and were less likely to seek early
diagnosis and treatment (Nazario, Figueroa-Vallés, Rosario, 2000;
O'Malley, Kerner, Johnson and Mandelblatt, 1999; Laws and Mayo,1998).
In Opposition: Physical Disability
The prevalence of functional
limitation and disability were higher for Puerto Ricans and Dominicans
in comparison to EA women in the same geographic area of Massachusetts
in 1998. Women demonstrated more physical limitations than men, and that
Puerto Rican and Dominican women demonstrated more limitations than EA
women. Additionally, it was also noted in this study that Puerto Rican
men demonstrated more disability than EA men ( Tucker, Falcon, Bianchi,
Cacho, and Bermudez, 2000).
In Opposition: Health
Insurance and Access
Risk for chronic disease
and injury among minorities vary both intra- and interstate. Contributing
to this risk is low rates of health insurance and poor health care accessability.
For example, Latinas and Latinos were more likely than EAs to report poor
access to health care, such as no health-care coverage and cost as a barrier
to obtaining health care. They were also more likely to report fair or
poor health status - obesity, diabetes, and no leisure-time physical activity
- than EA women(Bolen, Rhodes, Powell-Griner, Bland, and Holtzman, 2000).
Approximately 93% of all
people with diabetes have health insurance coverage of some kind - private
(73%), medicare (58%), medicaid (15%), veterans (5%). Approximately 54%
had multiple coverage. However, a much greater proportion of AA and EA
had coverage than did Latinas and Latinos. This trend held true for
all insurance coverage (Harris, 1999).
In Arizona, Latinas and
Latinos (26.2%) are twice as likely as EA (11.0%), to not have health insurance
(Bolen, Rhodes, Powell-Griner , Bland, and Holtzman, 2000).
All
in Favor Speak Now
As mentioned above, a review
of the literature revealed only a limited number of articles that spoke
directly to the EP. Below are those that speak in favor of the issue, or
which vacillate on the issue, through various types of illness and health
topics.
In Favor: Heart Disease
Where coronary and ischemic
heart disease is concerned, Latina/o are substantially less at risk than
either EAs or AAs:
"While coronary heart disease
is for Latinos, as other Americans the leading cause of death, the mortalities
rates are much lower than Non-Hispanic whites. Comparative mortality rates
per 100,000 for CHD, taken from the Analysis of Health Indicators for California's
Minority Population exemplify variation among Latinos. Several studies
verify lower cardiac mortality rates compared to non-Hispanic whites. Although
risk profiles ( Type A personality, obesity, Diabetes, hyperlipidemia,
hypertension, lack of exercise) are similar or unfavorable compared to
non-Hispanic whites, Mexican-American men generally are less likely to
have electrocardiographic evidence of myocardial infarction and exhibit
ischemic mortality rates 20-25% lower than whites (LatinoMed.com, 2000).
The CHD rates, normalized
by 100,000, and for age, according to LatinoMed.com (2000) are as follow
for: Mexican-American 88, Puerto Rican 94, Cuban American 92, EA 121, and
AA 188. The difference is dramatic. It is posited that Latinas/os may have
an unidentified protective factor which may be genetic (Diehl, 1989; Friis,
1981; Stern, M.P. 1985).
In Favor: Mother and Child
Outcomes
The greatest number of studies
demonstrating some facet of the EP are studies to do with mother's good
health, low use of illegal or harmful substances, and beneficial nutritional
habits before and after birth, the low incidence of preterm births, and
high birth weight (Fuentes-Afflick, et al, 1999). In most of these studies
Latinas quit smoking, stop drinking alcohol, and stopped taking drugs during
gestation (Schaffer, Velie, Shaw, Todoroff, 1998). Additionally, Latinas
also had excellent health outcomes despite having inadequate, or no, conventional
prenatal care (Higgins and Burton, 1996).
High number of births, low
birth weight and high infant mortality, are usually correlated with the
mothers poor health or associated risk factors. Latinas have one of the
highest birth rates among all women in the United States. Their birth rate,
per 1,000 of women of reproductive age, is an average of 107; with about
116 for Mexican American, 90 Puerto Rican, 50 Cuban, and 107 for other
South American women. This compares to about 64 for the general Unitedstatian
population (Becerra, J.E,. 1991).
Child bearing, then, appears
to demonstrate the EP concerning Latinas. There appears to be an inverse
correlation between low and moderate birth weight babies delivered to Latinas
and the mother's prenatal care, as well as at-risk factor for poor birth
outcomes - high unemployment, high single head of household status, high
incidence of not having prenatal care, etc. (Hajat, Lucas, and Kingston,
2000; Fuentes-Attlick, et al, 1999; Higgins and Burton, 1996).
Acculturation has been used
as a measure of inverse proportion for the EP; the more acculturated the
Latina, the worse the health outcomes (Balcazar and Krull, 1999). In an
examination of 4,404 births to Mexican-born and United States-born Mexican
Women it was found that foreign-born Latinas who spoke English at home
appeared to exhibit better birth outcomes than United States born Latinas
who spoke Spanish at home. This would seem to go against the usually held
belief that the Latina's culture was the primary factor in the EP (English,
Kharrazi, and Guendelman,1997).
It was found that foreign-born
Latinas who spoke English at home usually came from higher SES in their
native country and they tended to adhere more closely to their root culture.
United States-born Latinas who spoke Spanish at home tended to be from
lower socioeconomic, rural areas in marginalized communities that had adopted
poverty-driven risk behaviors such as subrosa barrio cultures (English,
et al, 1997).
In Favor: Mental Health
The National Institutes
of Mental Health (NIMH) says prevalence of mental illness is estimated
at about 20 percent of the U.S. population. That means millions are affected.
This is an estimate from two epidemiologic sources: the Epidemiologic Catchment
Area (ECA) study of the early 1980s and the National Co-morbidity Survey
(NCS) of the early 1990s. The National Institute of Health (NIH) states,
regarding epidemiological research for all ethnicities in the United States,
and referring specifically to depressive states in Latinas subgroups, that
"Prevalence information for other racial and ethnic groups is not definitive...."
However, NIH also says that depression is less for EAs and Latinas/os than
for Afro-American. NIH does NOT give incidence or prevalence. (National
Institute of Health, 2000).
In the United States, then,
there are fewer Latinas exhibiting or reporting depression than other ethnicities
- such as EA or AA women in the United States. Latinas report fewer incidences
of depression, and/or seek out less assistance for depression from traditional
medical service areas such as doctors, hospitals, mental health centers,
or health clinics(Nakamura, 1999). If the prevalence level of depression
in Latinas has an inverse proportion to risk factors for depression, as
found Nakamura (1999), then the EP exists for depression also.
By way of comparison with
EA women, studies seem to support the EP: Latinas seem to evidence the
same or less mental illness and depression than EA women. This may be due
to cultural inculcation in Latinas and/or modes of release and expression
through family and community. In Latinas, these modes of expression generally
permit more and open communication than in the EA culture (Nakamura, 1999).
As such, it would appear
that an argument can be made for depression similar to the argument that
is made in child bearing matters for Latinas: Latinas' culture may
have a preventive or even curative component on these illnesses or medical
situations.
In Favor: Cancer
In direct opposition to
the material presented concerning Latinas experiencing more cancers, the
Cancer Foundation chart of cancer incidence from 1990 to 1997 (Appendix
B) show that Latinas have lower rates of cancer (240.9 for all cancers)when
standardized by 100,000 population, than either EA (352.4) or AA (337.4).
The only higher instances were cancer of the cervix, where Latinas exhibit
higher rates than both EA and AA: is in(15.4, 8.4, 11.7 respectively).
Interestingly, Latinos also have a cancer rate which is much lower than
either EA men or AA men.
In Favor: Culture Confianza
For example, La Luz (1997)
found that the outstanding preventive difference keeping Latinas out of
prison was one of culture and community structure. Echoed over and over
again throughout the literature, relative to the Latina and Latino community,
was the solidarity engendered by the family-centered sense of community
felt within the various Latina and Latino enclaves across the United States:
confianza (La Luz, 1997). The sense of protectiveness and belonging
led to a tightly knit network community structure. The confianza
structure was reinforced by a very real sense of being, at best, marginal
outside the barrios (Heyck; 1994, Castillo, 1995; Cervantes 1996; Gonsalez,
1996; Kanellos, 1997, 1994).
The utter sense of trust
and faith (confianza) in the family and by extension, along with
confianza
in the immediate community at large (reinforced by marginality) acted as
a kind of insulation against the outside world. This confianza was
built on unconditional family-centeredness, on the principal that children
come first. That the family, children, and women (in that order) had to
be protected at all costs from any and all threats and dangers, whether
internal or external (Kanellos, 1997, 1994; Heyck, 1994; Cervantes, 1996;
Hayes-Bautista, et al, 1994).
Whether or not it is phenomenological
cultural construct, or some other determinates that account for the EP,
at least in prison rates and birth outcomes, remains to be conclusively
determined. However, it is important that some definitive answers are found
to address the needs of such a large population, a population that makes
up more than five percent of the entire population of the United States.
Others have said, that there
is need to design research that will test the theory that it is socioeconomic
status rather than race or gender that is really at work (Nakamura, 1999;
Holzer, Swanson, Shea, 1999; Knight, Virdin, Ocampo, and Roosa, 1994; Weissman,
Bruce, Leaf, Florio, and Holzer, 1991).
A
Qualitative Example
The issue has been examined
pro and con, though admittedly not exhaustively, through published research
articles. It is fruitful now to introduce a qualitative example of the
EP.
Marcia, a descended
of Senegalese slaves, Caribe Indians, Spanish invaders, and several other
ethnicities, was a typical
Puertorriquena. In essence, a Latina.
She lived in poverty most of her life. She worked at home, in New York
City, taking care and raising seven children, and several grand children
in the Latina/o tradition.
Marcia was very proud of
the fact that as a young women in Puerto Rico, she worked as a maid in
the Caribe Hilton in San Juan. She also worked rolling cigars, and cutting
sugar cane, but the job she always bragged about was the maid's job at
the Caribe Hilton. She believed that it was an honor to have been permitted
in to such an opulent place to work. It was prestigious and lucrative employment
to her.
Outside of the usual and
customary mild diseases - flues, colds and childhood diseases - she was
not seriously ill until her late sixties. From all I have read, Marcia's
experience with the health system in the United States, is typical of what
Latinas have suffered here (Cofer, 2000; Hogue, Hargrave, and Collins,
2000; Bayne-Smith, 1996; Lambety and Coll, 1994). She suffered a great
deal of discrimination. Three examples will suffice to illustrate the point:
In
Summary
An attempt has been made
to illustrate qualitatively the so called EP. Also research was presented
on both side of the argument. As such, according to the literature present
against the EP, Latinas have a higher incidence and prevalence of cancer,
diabetes, obesity, stroke, high blood pressure, and physical disability,
than do EA women (Nazario, et al, 2000; Tucker, et al, 2000; Flagg, 1999;O'Malley,
et al, 1999; Law, et al, 1998; Kattapong, et al, 1996; Kattapong, et al,
1997; Hazuda, et al, 1988; Samet, et al, 1988). Latinas also have poor
access to health services and insurance coverage which contributes to the
former (Bolen, et al, 2000). These conclusions would certainly seem to
put the lie to the EP. Or do they?
On the other side of the
argument, Cervantes' (1996) findings directly conflict with others for
such processes as cancer, diabetes, obesity, stroke, high blood pressure,
and abusing drug related behaviors. His finding also buttress the other
findings about Latinas appearing to exhibit excellent birth outcomes despite
high risk factors and adverse environmental conditions, and they present
less mental health problems and depression in particular, than EA women
(Hajat, et al, 2000; Namamura, 2000; National Institutes of Health, 2000;
Balcazar, et al, 1999; Fuentes-Afflick, et al, 1999; Schaffer, et al, 1998;English,
et al, 1997; La Luz, 1997; Higgins, et al, 1996; Guendelman and Abrams,
1995; Wagner-Echeagaray et al, 1994; Marin et al, 1993; Markides,1993;
Sorlie et al, 1993; Becerra et al, 1991; Marcus and Crane, 1985). The Cancer
Foundation also weighs in on the side of the EP by showing in their charts
that over a 9 year period (1990 to 1997, inclusively) that Latinas had
with only one exception, lower rates of cancer than either EA or AA women.
The findings in favor of
the EP seem to contradict those that are against it. A new hypothesis based
on qualitative analysis, quantitative research, and a social medical framework,
will demonstrate the fallacy of the epidemiological arguments pro and con.
Future
Direction
One of the processes that
must be undertaken is to dissect each and every study on the issue
of the EP for confounding variables, for poor design, and for rigor. In
this manner, some clear literature direction my be found that can be used
to buttress the hypothesis presented here, from a social medical framework.
Equally, as important, or
possibly more so, is to conduct social science epidemiological research
in several enclaves in the United States and Canada, using the epidemiological
methodologies of social medicine describe above. I would propose choosing
X amount of enclaves, and administering the surveys - individually and
group - and conducting individual and group meetings to confirm and readjust
the questionnaire findings. It would be an extensive project, but one well
worth the effort.
1. There is some
controversy of the uniqueness of this group, see the section on "disaggregation."
2. I use the term
"exploited" and "exploiter" nations, instead of the commonly used terms,
"developing nations" or "third world nations," as I believe the terms are
more descriptive of the dynamics in the world today, and they are more
in keeping with the ideological represented in this paper.
3. Throughout
this paper "social medicine" is used, with the understanding that it encompasses
both the terms "social and collective medicine."
4. Instead of the misleading
term "American" which predominates in the medical literature of the United
States when speaking of the United States of America, the literal translation
of "Unitedstatian" from the Spanish word "Estadounidense" is used throughout
this paper.
