Hormones and Resistance Exercise
By Derek Marks, M.S., and Len Kravitz, Ph.D.
Study Reviewed:
Taylor, J. M., Thompson, H. S., Clarkson, P. M., Miles, M. P., and De Souza, M. J. (2000). Growth hormone response to an acute bout of resistance exercise in weight-trained and non-weight-trained women. Journal of Strength and Conditioning Research, 14(2), pp 220-227.
INTRODUCTION
Hormones, such as human growth hormone and testosterone, play a large role in the muscle hypertrophy and strength gained resulting from resistance exercise. While increases in testosterone levels are attributed to the hypertrophy and strength gained in men, it is still unclear how women are able to respond similarly to resistance training in the absence of increased testosterone. The purpose of this article is to review the function of hormones and a recent study exploring the acute responses of growth hormone to an acute bout of resistance exercise in weight-trained and non-weight-trained women.
ENDOCRINE SYSTEM and HORMONES
The endocrine system helps provide stability to the body’s internal environment through the release of hormones. Hormones are substances secreted from a tissue (mainly endocrine glands) that exert a biologic response on itself or other cells, and affect almost all aspects of human function. They regulate growth, development, and reproduction, and augment the body’s capacity for handling physical and psychological stress. Hormones differ in how they affect their target cells, and can be classified into three categories: amine, peptide, and steroid.
Amine hormones are derived from amino acids, while peptide hormones are structured by peptide bonds between multiple amino acids. Amine and peptide hormones are soluble and are transported in blood plasma in solution. The water-soluble characteristics of amine and peptide hormones make them easily removed from the circulation allowing only a short time (minutes) to exert their function.
Steroid hormones are not water-soluble and therefore must be bound to plasma proteins to be transported to their target tissue. The protein binding complicates the activity of steroid hormones, delaying the time to stimulate a biological response.
HORMONE ACTION
The major function of hormones is to alter the rates of specific cellular reactions of specific target cells. This is accomplished by altering the rate of intracellular protein synthesis, changing the rate of enzyme activity, modifying plasma membrane transport, and by inducing secretory activity (Robergs and Roberts, 1997).
Hormones are able to reach virtually all tissues because they travel in the blood. However, the ability for a target tissue to respond to a hormone depends on the presence of specific receptors in or on the tissue. Amine and peptide hormones exert their action on target cells by binding to specific receptors on the membrane of the target tissue. In response to the hormone binding, a molecule called a “second messenger” is produced, which then stimulates a cellular response. The most common of these second messengers is cyclic adenosinemonophosphate (cyclic AMP). For example, in bone and muscle cells, the cyclic AMP produced by the action of growth hormone binding activates anabolic reactions so amino acids can be synthesized into tissue proteins.
Steroid hormones do not bind to the membrane of the target tissue, but instead pass through it and then bind to a specific cytoplasmic steroid receptor in the cell, which then migrates to the nucleus. Once there, it enters the nucleus and initiates the nuclear and cytosolic events required for the synthesis of specific proteins.
HORMONE SECRETION
Control of hormone secretion must be rapid in order to meet the demands of changing bodily functions. Hormone secretion is usually pulsatile in nature and constant hormone release rarely exists. The predominant hormonal control mechanism is referred to as “negative feedback.” This is very similar to how a thermometer works in your home. For example, an increase in blood glucose levels causes the release of insulin by the pancreas. Insulin action causes an increase in glucose uptake, resulting in lowered blood glucose levels. The decrease in blood glucose “sends a feedback message” to the pancreas, resulting in the halting or decrease in the release of insulin. The end result of insulin action is the inhibition of its own release as the body reaches its desired homeostasis.
HORMONES and EXERCISE
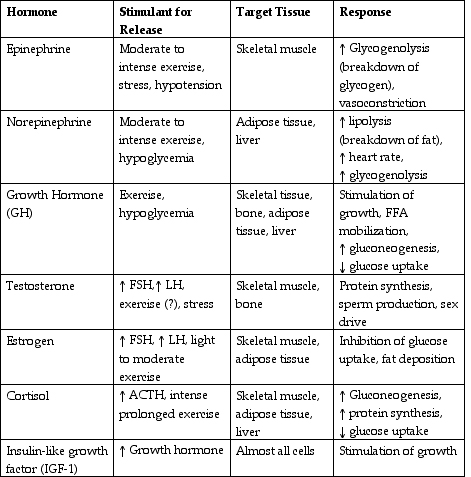
Hormone release can be stimulated by both external and internal stresses to the body. Adapting to acute exercise causes an increase in the secretion of many hormones. Several of the main hormones related to exercise and their responses are listed in Table 1.
RECENT INVESTIGATION
It is well documented that the secretion of anabolic steroids results from resistance training, yet it is not clear why women exhibit similar responses to training (compared to men) in the absence of increased testosterone levels (Taylor et al., 2000). In a recent study by Taylor and colleagues, investigators examined the differences in growth hormone (GH) response to acute bouts of resistance exercise in weight-trained (WT) and non-weight-trained women (NWT). Growth hormone is responsible for increasing protein synthesis and for mediating the release of insulin-like growth factor (IGF-1), which is another potential anabolic factor (Taylor et al., 2000). They hypothesized that women with weight training experience would have a greater GH response to the exercise stimulus than the non-weight-trained women (Taylor et al., 2000).
The subjects included twelve healthy, eumenorrheic (normal menstruating), ovulatory women. Women assigned to the WT group had at least one-year of consistent weight training experience, while the NWT women had no regular weight training experience for at least six-months prior to the beginning of the study.
As part of the experimental design, the subjects were first familiarized with the exercise protocol, and their 10-repetition maximum was determined for the various exercises included in the protocol. The exercise protocol consisted of three sets of 10 repetitions for seven different exercises (bench press, leg press, seated shoulder press, leg extension, lat pulldown, biceps curl, and triceps pushdown) with one-minute rest periods between sets and exercises. Blood samples for hormone assays were taken ten and five minutes prior to exercise, and immediately, 5, 15, 30, and 60 minutes after exercise. All testing was performed 2 to 4 days after the onset of menses. This was done to help minimize the estradiol effect (the most potent naturally occurring estrogen). Diet, exercise, and supplementation were controlled for the day prior to testing.
Growth hormone levels were analyzed in absolute terms (i.e. which group had greater GH level at a specific time period) and in cumulative terms (i.e. which group had a greater GH response to exercise from pre-exercise to 60 minutes post exercise). The WT women had lower pre-exercise GH levels compared to NWT women. Additionally, the GH values measured immediately post-exercise and five minutes after were lower for the WT women. However, the overall GH response to the acute bout of resistance exercise was greater for WT women. What this means is that when using the pre-exercise GH level as a baseline value for each group, the WT women had a greater overall increase over the duration of the study (pre-exercise to 60 minutes post-exercise) in GH in response to exercise.
CONCLUSION
These findings demonstrated that both WT and NWT women have an acute rise in GH levels following resistance exercise, however, the WT women were able to sustain the increased GH levels for a longer period of time. The exercise protocol used in this study provided sufficient stimulus to cause GH levels to increase in both groups. Exercise variables contributing to GH release include intensity, load, rest interval, and the amount of muscle mass utilized. Since both groups used the same intensity, load, and rest period the differences in response may be explained by the WT women utilizing greater amounts of muscle mass during exercise. It could be assumed that due to greater exposure to resistance training, the WT women had greater amounts of lean body mass, and that training exposure also allowed for a greater relative recruitment of their motor unit pool when exercising (Taylor et al., 2000). This in turn stresses more sarcolemma of muscle, resulting in increases in anabolic hormone levels. Thus the authors suggest that the magnitude of hormonal response is related to the amount of muscle tissue stimulated.
PRACTICAL APPLICATION
The researches suggest that women should be encouraged to engage in resistance exercise, since there may be an influential effect of growth hormone response in women attempting to develop strength and power. However, further investigations are necessary to fully describe the relationship between hormonal responses and resistance-training in women.
Table 1. Main functional responses to exercise and glandular tissues and hormones involved in acute adaptation in men and women (from Robergs and Roberts, 1997). |